
 Discussion
Discussion
Types of hemophilia
Last updated April 11, 2025, by Marisa Wexler, MS
 Fact-checked by Joana Carvalho, PhD
Fact-checked by Joana Carvalho, PhD
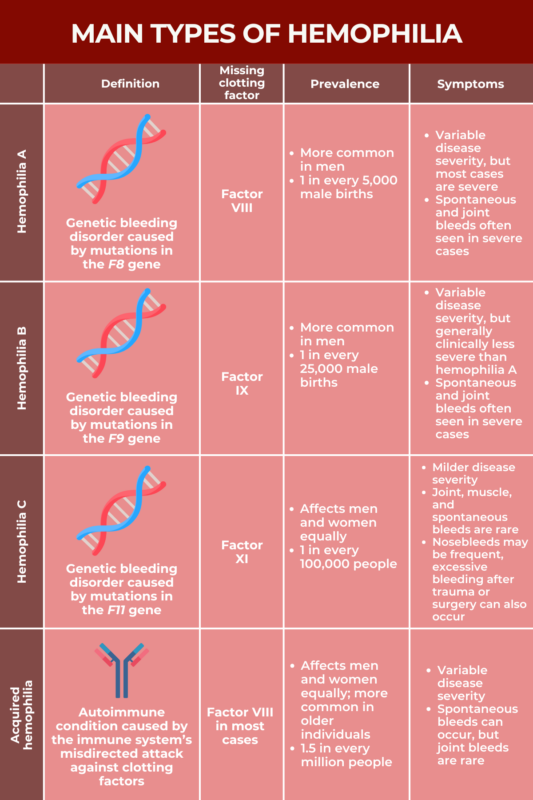
There are several types of hemophilia, a rare bleeding disorder wherein the blood fails to clot properly. Hemophilia A and B are the most common types, while hemophilia C is comparatively rare.
All types of hemophilia are characterized by the lack or dysfunction of blood clotting proteins called clotting factors. Generally, the type of hemophilia a patient has depends on the specific clotting factor that is missing.
Most cases of hemophilia are caused by mutations in the genes that provide instructions for making specific clotting factors, impairing the body’s ability to produce a sufficient amount of functional clotting proteins. There’s also an acquired form of hemophilia where the immune system accidentally attacks and destroys certain clotting proteins.
Comparison of hemophilia types
Each type of hemophilia is marked by the lack or dysfunction of a specific clotting factor. While a deficiency in clotting factor VIII (FVIII) is the underlying cause of hemophilia A and most cases of acquired hemophilia, a deficiency in clotting factor IX (FIX) and clotting factor XI (FXI) are the root causes of hemophilia B and C, respectively.
Besides being associated with distinct clotting factors, the different types of hemophilia also differ in prevalence, with hemophilia A being the most common and acquired hemophilia being the rarest.
Disease severity and hemophilia symptoms also vary across the different hemophilia types. For instance, more severe disease and joint bleeds are more commonly seen in patients with hemophilia A or B, while people with hemophilia C generally have milder disease manifestations, with spontaneous bleeding and joint bleeds happening rarely. Joint bleeds are also not common with acquired hemophilia.
There are several hemophilia treatment options for the different hemophilia types. In general, treatments that can help prevent or control bleeds are the most important aspect to consider across all types. Such treatments may include factor replacement therapies, nonfactor replacement therapies, and even gene therapy. Specialized care and management are also available to patients at hemophilia treatment centers.
Hemophilia A
Hemophilia A, known as classical hemophilia, is caused by a FVIII deficiency due to mutations in the F8 gene, which provides instructions for making FVIII. It’s estimated to occur in about 1 out of every 5,000 male births and is the most common form of hemophilia, accounting for approximately 80% of all cases.
In people who don’t have hemophilia, FVIII activity typically ranges between 50% and 150% compared with normative values. In people with mild hemophilia A, FVIII activity levels usually range between 5% and 40%. In moderate hemophilia A, FVIII activity levels range between 1% and 5%, and fall to less than 1% in severe hemophilia A.
About 60% of people with hemophilia A have the severe form of the disease. People with severe hemophilia A commonly have excessive or prolonged bleeds without any apparent cause that often occur in the muscles or joints. Those with moderate or mild hemophilia A don’t typically have spontaneous bleeding episodes, but they can experience excessive bleeding following an injury or after surgery.
Because people with more severe hemophilia tend to have more frequent bleeding problems, they are generally diagnosed earlier in life.
Hemophilia A is typically treated with replacement therapies that provide a working version of the missing FVIII protein, the goal being to lower the risk of bleeds and control active bleeds. In recent years, gene therapy that works to deliver a working version of the F8 gene to cells has become available for some people.
Who develops hemophilia A?
The F8 gene is found on the X chromosome, one of the two sex-determining chromosomes. People who are biologically female have two X chromosomes. Biological males have one X and one Y chromosome.
Hemophilia A only develops if a person doesn’t have a working copy of the F8 gene. Consequently, it’s much more common in men, who only have one X chromosome, than in women, who have two and for whom one working copy can compensate for a mutated copy.
In about 70% of the cases, the mutation that causes hemophilia A is inherited from a person’s parents, usually the mother, since males inherit their single copy of the X chromosome from their mother. In the remaining cases, mutations develop de novo, meaning a child has a mutation that arises spontaneously, rather than being inherited from a parent.
Hemophilia A affects people of all races and ethnicities at roughly equal rates.
Hemophilia B
Hemophilia B is caused by a FIX deficiency due to mutations in the F9 gene, which provides instructions for making FIX. This type of hemophilia is also known as Christmas disease, after a 5-year-old boy named Stephen Christmas who, in the early 1950s, was the first person to be formally diagnosed with it.
Hemophilia B, the second most common type of hemophilia, is about five times less prevalent than hemophilia A, with estimates indicating it occurs in about 1 in 25,000 male births.
Like hemophilia A, hemophilia B can be divided into the same three categories of severity based on FIX activity levels. People with FIX activity levels ranging between 5% and 40% are said to have mild disease, while those with levels ranging between 1% and 5% have moderate disease. Those with FIX levels of less than 1% have severe disease. As with hemophilia A, spontaneous bleeds and joint bleeds are more common with severe hemophilia B.
Both hemophilia A and hemophilia B are marked by abnormal bleeding. While there can be a lot of variability from person to person, studies generally suggest that people with hemophilia B tend to have less severe disease than those with hemophilia A, even among patients with similar disease severity based on clotting factor levels.
Replacement therapies that deliver a working version of the FIX protein are typically used to prevent bleeding episodes and control active bleeds in people with hemophilia B. Recently, gene therapy that delivers a healthy copy of the F9 gene has become available for some people.
Who develops hemophilia B?
The F9 gene is located on the sex-determining X chromosome, thus, like hemophilia A, hemophilia B is much more common in men than in women.
A mutation inherited from the parents is the cause of about two-thirds of cases of hemophilia B, while the remaining one-third of cases arise due to spontaneous mutations. The disease occurs at similar rates across racial and ethnic groups.
There is also a rarer subtype of hemophilia B, known as hemophilia B Leyden, after the city in the Netherlands where it was first described. People with this subtype are born with virtually no FIX, but FIX levels gradually increase throughout life, reaching the lower limit of the normal range by midlife in some cases. Hemophilia B Leyden is estimated to account for 3% of all hemophilia B cases.
Hemophilia C
Hemophilia C, also known as Rosenthal syndrome, is caused by a FXI deficiency due to mutations in the F11 gene, which carries instructions for producing FXI. Hemophilia C is notably more rare than hemophilia A or B, affecting about 1 out of every 100,000 people.
People with hemophilia C generally have symptoms that are not as severe as those seen in people with hemophilia A or B. Unlike other forms of hemophilia, the degree of FXI deficiency is not necessarily tied to disease severity, meaning it’s not possible to predict symptom severity based on FXI levels with hemophilia C.
Unlike hemophilia A and B, joint, muscle, and spontaneous bleeding episodes are rarely seen in hemophilia C. However, patients with this type of hemophilia may have frequent nosebleeds, or experience excessive bleeding after trauma or surgery, such as following a tooth extraction.
Hemophilia C often doesn’t require treatment unless a patient is undergoing a surgical procedure where major bleeding is considered a risk. When treatment is needed, hemophilia C is usually managed with infusions of fresh frozen plasma (the noncellular component of blood) or with medications that slow the breakdown of blood clots, thereby helping to prevent blood loss.
Who develops hemophilia C?
Unlike the F8 and F9 genes, the F11 gene isn’t located on a sex-determining chromosome. Therefore, every person inherits two copies of the F11 gene, one from each parent. Severe hemophilia C will usually only develop if a person has mutations in both F11 copies. A person who carries only one mutated copy generally won’t have severe symptoms, but may still pass on the mutated gene to their children.
If two people who are both carriers of a faulty F11 gene copy have a child, there is a:
- 25% chance the child will inherit both mutated copies of the F11 gene and develop hemophilia C
- 50% chance the child will inherit one mutated gene copy and be a carrier
- 25% chance the child will not inherit any mutated copies of the gene and be healthy.
In some instances, just one mutated gene copy is sufficient to cause hemophilia C, though this is rare and usually doesn’t lead to severe disease. If a person with hemophilia C caused by one mutated copy of the F11 gene has children, there’s a 50% chance of passing the disease-causing mutation to their children.
Hemophilia C is more rare than hemophilia A or B, affecting about 1 out of every 100,000 people. Unlike other forms of hemophilia more common in men, hemophilia C affects men and women equally. Hemophilia C is also more common among Ashkenazi Jews, affecting about 8% of people in this ethnic group.
Acquired hemophilia
While most types of hemophilia are genetic bleeding disorders caused by mutations a person is born with, acquired hemophilia is an autoimmune disease that develops over a person’s lifetime. Acquired hemophilia is very rare, affecting an estimated 1.5 out of every 1 million people per year.
In acquired hemophilia, the immune system fails to recognize a clotting factor as a healthy part of the body. As a result, immune cells produce antibodies that attack the clotting protein as if it were an infectious agent, preventing it from functioning normally.
In most cases of acquired hemophilia, the immune system specifically attacks FVIII, the clotting protein that’s missing or is defective in hemophilia A. More rarely, acquired hemophilia also can develop as a result of an autoimmune attack targeting other clotting proteins.
The severity of acquired hemophilia can vary widely. Around 1 in 3 people with acquired hemophilia have relatively mild symptoms and don’t require specific treatment, but some patients do have frequent and serious bleeds, which can be life-threatening, especially if the condition isn’t diagnosed correctly and treated promptly.
Bleeds can occur spontaneously for no apparent cause in acquired hemophilia, but unlike other types of hemophilia, joint bleeds are rare.
Because it’s so rare, there aren’t well-established guidelines for treating acquired hemophilia, so treatments tend to be highly tailored to the individual patient. That said, treatment for acquired hemophilia generally has two main goals. They are:
- control bleeding (e.g., bypassing agents)
- reduce or eliminate the production of antibodies that target clotting factors (e.g., immunosuppressive medications, corticosteroids).
Who develops acquired hemophilia?
Acquired hemophilia occurs at similar rates in men and women and, while it can develop at any age, it most commonly occurs in the latter decades of life. It’s estimated that about 80% of people with acquired hemophilia are older than 65. It arises in people without a family history of a bleeding disorder.
In about half of the cases, acquired hemophilia develops in people who already have other underlying health problems, such as:
- autoimmune diseases, including lupus, rheumatoid arthritis, myasthenia gravis, or multiple sclerosis
- cancer, including lung, prostate, pancreas, breast, and several types of blood cancers
- skin conditions, such as psoriasis, pemphigus, and epidermolysis bullosa
- infectious diseases, such as hepatitis B and C
- diseases involving the gastrointestinal tract, such as inflammatory bowel disease
- transplant-related disorders, including chronic graft versus host disease
- lung diseases, such as asthma or chronic obstructive pulmonary disease.
Acquired hemophilia also can develop as a complication following childbirth, which accounts for nearly 10% of cases. It also may develop as a reaction to blood transfusions or to certain medications, including some antibiotics and nonsteroidal anti-inflammatory drugs.
No specific cause or underlying health condition can be identified in about half the patients, however.
Hemophilia News Today is strictly a news and information website about the disease. It does not provide medical advice, diagnosis or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.

Related articles
-
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion